
Does every meniscal tear require surgery?
Should the meniscal tear which is decided for operation be immediately operated? Meniscuses are the…

Anatomy of Anterior Cruciate Ligament
Anterior cruciate ligament is one of the main ligaments that provide for stabilization of the knee joint. It is located at the middle of the knee joint and prevents the knee from shifting forward; when it is totally torn, the patients come to the physician with the complaint of discharge at the knee.
Knee ligament injuries mainly occur during twenties and thirties.
Risk factors in anterior cruciate ligament tear:

1- Anatomic narrowness in the area where cruciate ligament binds
2- Joint laxity (widespread ligament looseness)
3- Makign sports on rough ground.
4- Female gender: (risk of anterior cruciate ligament injury in women performing the same sports is 4-8 higher than men)
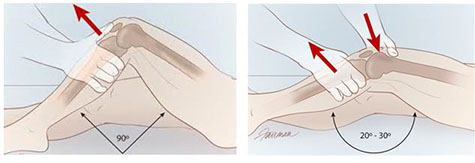
Mechanism of Occurrence:
This arises frequently when the body rotates on the knee when the foot is fixed on the ground.
This arises during sudden slow down for changing direction while running in persons engaged in basketball or football.  Besides, an uncontrolled loading on the knee after bouncing could lead to tear of cruciate ligament. Meniscal tear frequently accompanies the anterior cruciate ligament tear.
Besides, an uncontrolled loading on the knee after bouncing could lead to tear of cruciate ligament. Meniscal tear frequently accompanies the anterior cruciate ligament tear.
In the absenceof anterior cruciate ligament, the biomechanics and kinematics of the knee joint is distorted, which leads to abnormal loads on meniscus and knee joint cartilage, as a result of which degenerative arthritis (joint surface damage) occurs.

Complaint of the Patient:
The story of the patient is typical, where the complains change depending on whether it is acute or chronical.
In acute cases (newer than 3 weeks), basic complains include knee pain, swelling and restriction of active movements, failure to make the knee totally smooth, feeling of insecurity, walking by limping and being in need of walking support. The complaint of discharge in knee is not frequent since walking is not performed much due to pain. Some patients may hear the sound of breaking as the knee rotates during sports.
In chronical cases (older than 3 months): Patients apply to physician suffering from failure to run and make sports, feeling of insecurity in sudden bouncing, stopping and rotating movements and discharge. Swelling episodes could be seen on the knee with the third frequency. Meniscal tear could be found at a rate of 50% in patients who have anterior cruciate ligament tear. Locking and pain complains could be seen due to meniscal tear. Whereas patients with anterior cruciate ligament tear could perform sports, significant performance losses could occur.
Whereas cartilage damage could occur in the acute period in anterior cruciate ligament tear, there may be an increase in cartilage damage rate depending on the frequency of discharges on the knee in chronical period. It is known that meniscuses and joint cartilage is protected as the anterior cruciate ligament is repaired.
How is it diagnosed?
Examination: In acute tears, the patient comes with a swelling on his knee, the knee is highly painful and tensile, it may sometimes not be possible to perform specific examination tests due to pain.
Detailed knee examination is performed on the patient who comes in chronical period; meanwhile specific tests are applied for anterior cruciate ligament tear.
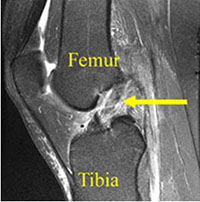
Imaging Methods:
Classical conventional X-Ray: Whereas acute anterior cruciate ligament tear does not give any finding in diagnosis, anterior cruciate ligament tear could be doubted with some indirect findings in case of chronical tears. The easiest imaging method which gives the most clear finding today is MR.
How should anterior cruciate ligament tear be treated?
Conservative (no surgery)? Surgery?
As a result of developments in surgical technologies in recent years, it is indicated that clinical results may lead to unacceptable results in many cases in patients who are not operated. Is surgery the only option? Whereas surgical treatment is the only option, it is the best option in terms of functional results.
What are the conditions to pay attention while making the decision for surgical treatment?
1-The most important factor is the age of the patient.
Aged 12 to 20:
Since the level of activity is high in this age group, surgical treatment is the best option.
Aged 20 to 40:
It is acknowledged that non-surgical methods are not beneficial in this active age group, and that the best option in individuals who make sports is surgery.
Aged 40 to 60:
The main criteria in these patients is the degree of sportive activity rather than age. Whereas in particular non-surgical treatment methods are successful in individuals aged above 40 who do not make sports, surgical treatment option is leading in persons who engage in high level of activity such as running or tennis.
2-Strength of injury and accompanying additional injuries:
If there are other ligament or meniscal tears than anterior cruciate ligament, surgical treatment is preferred.
3-Activity type and level: Surgical treatment should be the first option for those who make sports regardless of the age.
What should the timing of surgery be?
If the patient has appeared before the physician in the acute period (first three weeks); he should be immediately operated if he is a professional sportsman, if not, 3 weeks should be waited if there is no meniscal tear to be repaired. Edema occurs in structures surrounding the knee with the effect of trauma that creates the tear; when the surgery trauma is added on this, joint stiffness could develop though rarely in the postop period. In professional sportsman, immediate surgical treatment is recommended in order to ensure return back to sports at the earliest convenience possible.
Patients who are diagnosed in the chronical period ( after 3rd month), could be operated at any suitable time.
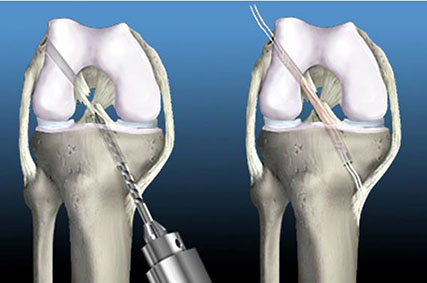
What Are Surgical Treatment Methods?
Anterior cruciate ligament repair is not a surgical method which could be treated by stitching the torn ligament end by end. Ligament transplantation is made in place of the torn ligament. There are 2 types of ligaments that could be used for ligament transplantation. First are the ligaments that are obtained from the body of the person (autograft), and the second are those obtained from the cadaver (Allogreft).
Frequently the autografts are used today due to the problems of fitting to the body and less resistance. However, allgrafts are used for weakening the existing structure in some sportsman.
Whereas autografts could be obtained from some different regions of the body, today mostly the back muscle tendons of the thigh (Hamstring) are used.
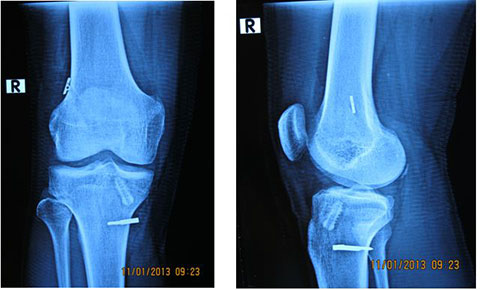
Hamstring tendons are located inside the bone tunnels opened inside the knee joint, and they are attached to the bone using various methods as well as arthroscobic method (closed surgery).
Complications?
The most frequent complications are the pains and bleeding in relation to the area where graft is taken. Although some complications could be seen during and after the surgery, bleeding, pain, infection, joint stiffness, loosening or breakage of the tendon applied could frequently occur.
Rehabilitation Following Surgery:
Rehabilitation in the repair of anterior cruciate ligament changes from patient to patient.
The reasons for this are the strength of fixing, type and location of the graft used, type of the surgical process and other reasons accompanying the injury.
Anterior cruciate ligament surgery is applied in our clinic to professional sportsman and those who do not have a sportive position.
The surgery is performed as arthroscopy method (closed method). The surgery could last for 60 to 90 minutes on average depending on whether there is meniscal tearing or any other additional lesion. The patient is hospitalized for 3 days for rehabilitation following the surgery and physical treatment is applied during this period.
 The patients stood up 6 hours following the operation and walked by applying partial load. Knee support could be prescribed to discharged patients for 20 days depending on the strength of Quadriceps muscle. Patients on desktop work could return to work at the end of 20 days, and this period could reach to 45 days in patients who are on foot work. Return to active competition sports is permitted 8 months later. The graft that is placed could reach to the maximum power 1 year following the surgery. It should be protected during this period.
The patients stood up 6 hours following the operation and walked by applying partial load. Knee support could be prescribed to discharged patients for 20 days depending on the strength of Quadriceps muscle. Patients on desktop work could return to work at the end of 20 days, and this period could reach to 45 days in patients who are on foot work. Return to active competition sports is permitted 8 months later. The graft that is placed could reach to the maximum power 1 year following the surgery. It should be protected during this period.

